Right upper lobe collapse – CXR/CT
This 70 year old man presented with haemoptysis.
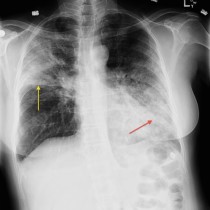
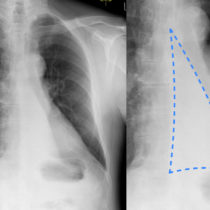
Chest radiograph performed on admission shows the typical appearance of right upper lobe collapse. There is an opacity in the medial aspect of the right upper zone that represents the collapsed upper lobe, which has migrated upwards and medially as a result. The horizontal fissure, indicated by the dashed line in the middle zoomed image, has migrated upwards and medially as well. There are further features of volume loss in the right side of the chest; the right hemidiaphragm is mildly elevated, there has been shift of the trachea to the right, and the upper right ribs appear closer together than their counterparts on the left. Also, the remaining right lung is relatively lucent when compared to the left as it has expanded to try to fill the space left by the collapsed upper lobe.
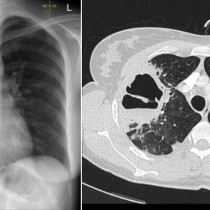
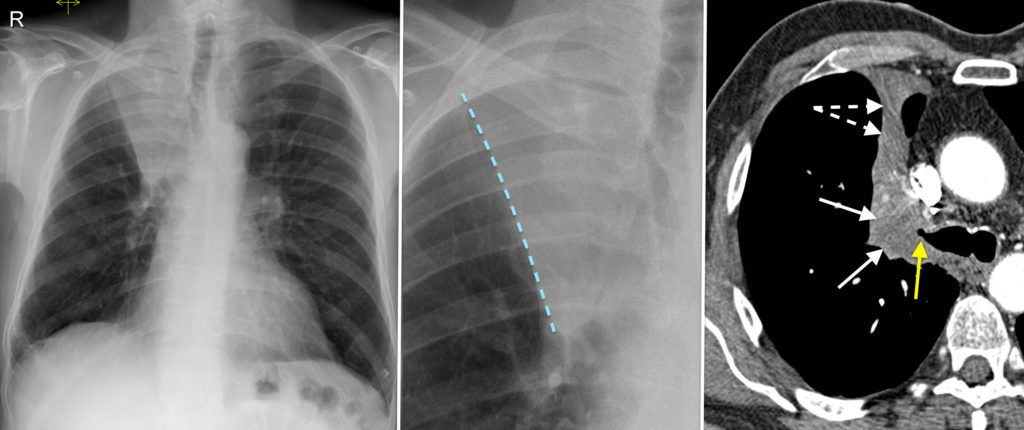
While there is a differential diagnosis for right upper lobe collapse that includes mucus plugs or potentially a foreign body, in an adult one should always be very suspicious of an underlying tumour. As a result, CT is performed routinely in these cases, and in this example it confirmed that there was a neoplasm at the right hilum (indicated by the white arrows on the CT image). You can see that the tumour has occluded the right upper lobe bronchus (yellow arrow), resulting in the lobar collapse. The displaced horizontal fissure is indicated by the dashed white arrows. Bronchoscopy was performed and a biopsy confirmed that this was a primary bronchogenic neoplasm.
Although not present in this case, the underlying hilar tumour is often a lot larger and can cause some bulging of the displaced horizontal fissure – this results in a lazy backwards ‘S’ shape to the fissure, and is called the ‘S-sign of Golden’.
You should note that left upper lobe collapse does not result in a similar appearance – instead, the classic radiographic finding is the presence of a ‘veil-like’ opacity throughout the left hemithorax, loss of distinction of the left heart border, with the addition of some of the signs of volume loss listed above.