Gastrostomy tube insertion (RIG)
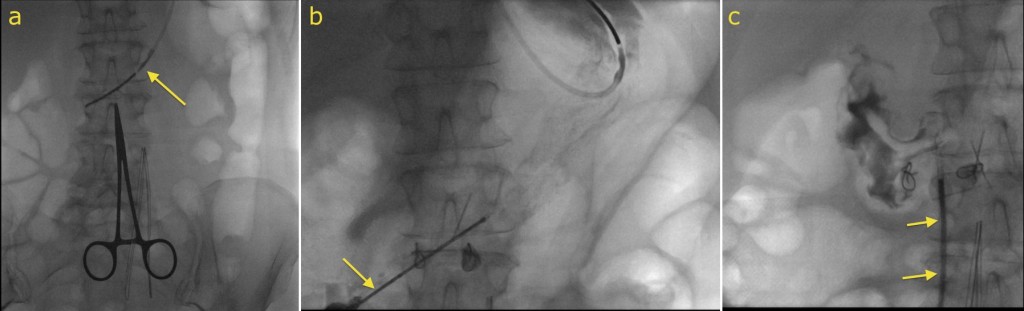
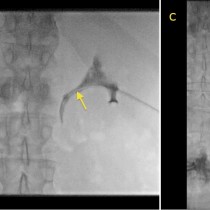
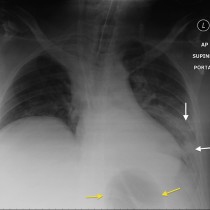
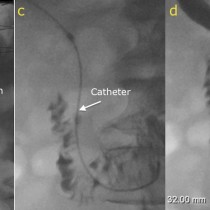
Radiologically-inserted gastrostomy (RIG). Indications for gastrostomy include patients with neurologic impairment who are unable to swallow without aspirating, patients who require long-term nutritional support (including some patients with CF), and patient with oro-pharyngeal or oesophageal malignancy. In this example, the patient had squamous cell carcinoma of the larynx and required a gastrostomy for feeding while undergoing radiotherapy (as this frequently causes impaired swallowing due to mucosal injury). Briefly, the technique for RIG involves the insertion of a nasogastric tube (arrow in image a). An artery clip has been placed on the patient’s epigastrium to plan an appropriate skin puncture site. In order to safely puncture the stomach percutaneously, it needs to be distended with gas. This is accomplished by blowing air through the NG tube. On image (b), the stomach is distended with air (and occupies much of the image), and an access needle has been inserted (arrow). Contrast has been injected to confirm that the needle tip is in the gastric lumen (you can see that it has flowed towards the gastric fundus, at the top right of the image). A guide-wire is passed through this needle, over which the gastrostomy tube is advanced (image c, arrow). The tube is held in place in the gastric lumen by inflating a small balloon at its tip.