Prostate cancer – MRI
This 69-year-old man with an elevated PSA and a clinical suspicion of prostate cancer was referred for an MRI of the prostate.
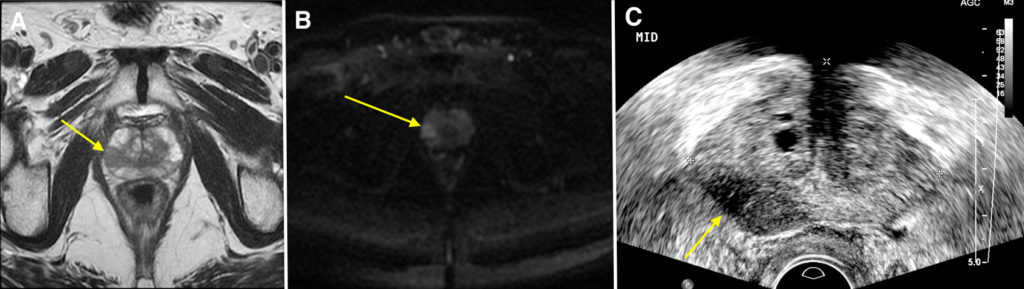
This identified a 2 cm tumour in the peripheral zone in the right apex. The patient underwent a targeted biopsy of the tumour under transrectal ultrasound guidance (TRUS) which confirmed a high grade adenocarcinoma.
The axial T2-weighted MR image (A) shows a dark or hypointense lesion (arrow) in the peripheral zone (which is usually bright or hyperintense). The lesion has corresponding diffusion restriction – seen as bright signal on the diffusion weighted image (B). These appearances are typical for prostate cancer. The majority of tumours are located in the peripheral zone.
In recent years, MR imaging of the prostate has significantly changed practice for the diagnosis and management of patients with prostate cancer. Patients with a mildly elevated PSA who have a normal MRI are unlikely to have clinically significant prostate cancer. MRI has an important role in the identification of suspicious lesions to target at biopsy. There are three methods that Radiologists can use to perform a targeted biopsy after an MRI shows a lesion of concern:
– Directly in the MRI scanner using special equipment
– Using fusion software that superimposes the lesion seen at MRI onto real-time TRUS images
– “Cognitively” by studying the MRI and finding that exact corresponding location on TRUS
In this case the patient underwent a “cognitively” targeted biopsy using TRUS (image C). On TRUS there was a corresponding hypoechoic abnormality visible on ultrasound which was helpful (arrow), however often the lesions cannot be seen on ultrasound.
MRI of the prostate also has an important role in staging patients with known prostate cancer who are being considered for potentially curative surgery (radical prostatectomy). For these patients MRI can identify extra-prostatic extension of the tumour, as well as pelvic lymph node and bone metastases.
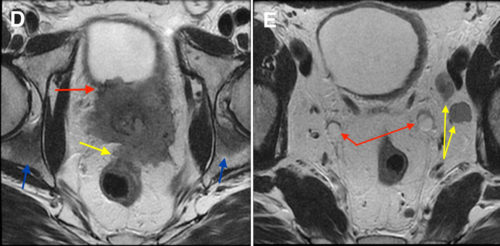
Images D and E below are from an MRI of a different patient with a locally advanced tumour which has replaced the entire prostate gland. There is invasion of the bladder anteriorly (red arrow) and the rectum posteriorly (blue arrow). There are bilateral ischial bone metastases (blue arrows), as well as left pelvic sidewall lymph node metastases (yellow arrows in image E). Note also the bilateral hydroureter (red arrows in image E) due to obstruction of the ureterovesical junctions by tumour.
Case contributed by Dr Ciaran Redmond.