Gallstone Ileus
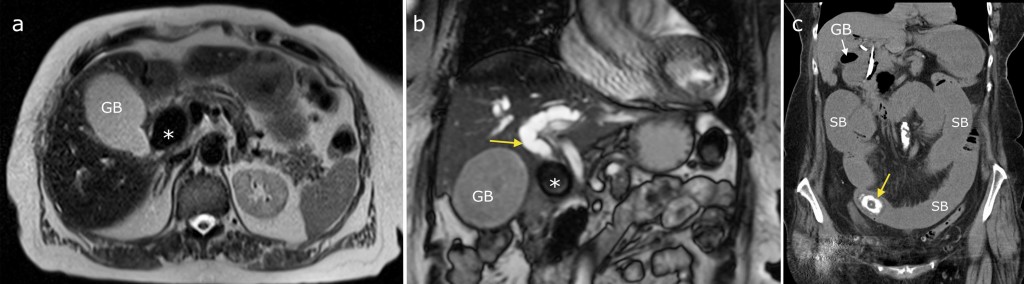
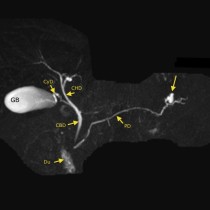
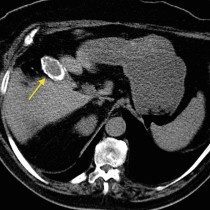
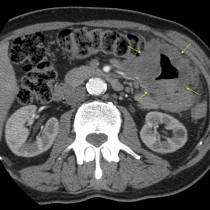
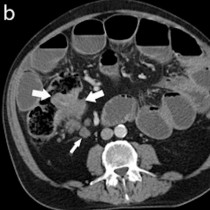
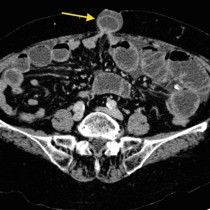
This unlucky patient presented with acute cholecystitis secondary to a large calculus impacted in the cystic duct. Following admission she became jaundiced and a follow-up ultrasound showed dilated intrahepatic bile ducts. An MRCP was performed to further evaluate this. Axial T2-weighted image (a) shows the dilated gallbladder, GB, as well as the large low signal calculus (*) in the gallbladder neck and cystic duct. Coronal image (b) confirmed that this impacted calculus (*) was the source of the patient’s biliary obstruction – the common hepatic duct (arrow) is markedly dilated as far as the calculus, indicating that the patient had developed Mirizzi syndrome. In this syndrome, the extrahepatic biliary tree is extrinsically compressed by a calculus or calculi in the cystic duct. This is often exacerbated by associated inflammatory changes. A CBD stent was inserted at ERCP however a few days later the patient developed symptoms of bowel obstruction, and dilated small bowel was visible on an abdominal radiograph. CT was performed (image (c)) and showed that the cause of the dilated small bowel (SB) was the gallstone (arrow) – it had eroded into the duodenum (a choledochoduodenal fistula) and then obstructed the distal small bowel. A laparotomy and enterotomy were performed, and the gallstone removed. A lot of trouble from one stone!