Embolization of superior mesenteric artery haemorrhage
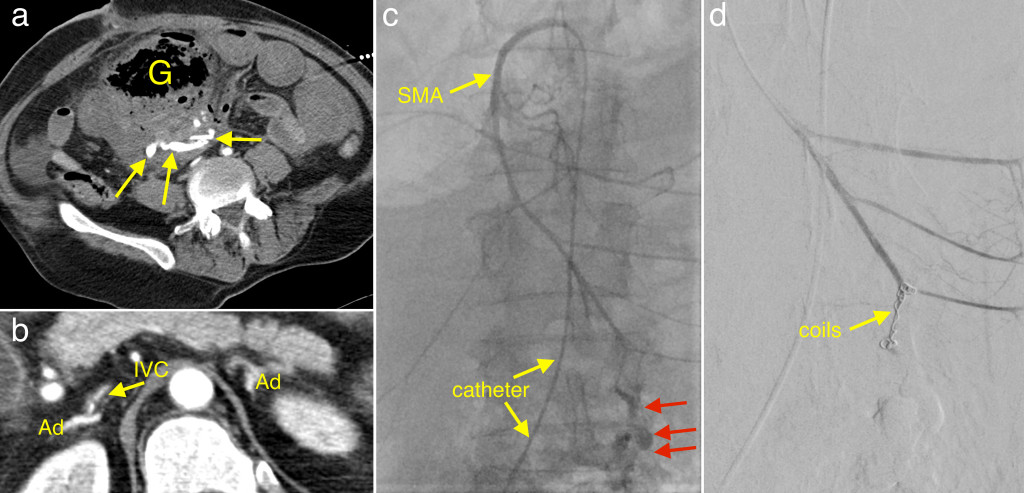
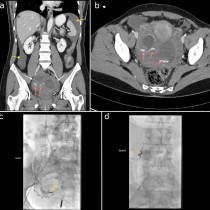
This man went into cardiac arrest a few days after a small bowel resection. He was resuscitated and brought straight to CT, where a large amount of gas was demonstrated adjacent to the resection site, indicating an anastomotic leak (image (a), labeled ‘G’).
Adjacent to this was a haematoma which contained some of the IV contrast that had been injected, indicating active extravasation (arrows). This contrast was extravasating from a defect in the distal superior mesenteric artery (SMA). At this stage the patient was profoundly hypotensive, despite vasopressors. We can guess this from the CT, which shows some of the characteristic features of shock – a slit-like IVC (image (b)), and hyperenhancing adrenal glands (Ad).
He was brought straight to the interventional radiology suite, and a catheter passed through the femoral artery and aorta and into the SMA. Image (c) shows the injected contrast pouring straight out of the distal aspect of the SMA (red arrows). Coil embolisation of the SMA was performed and image (d) shows that the contrast extravasation has ceased. This resulted in immediate stabilisation of the patient – his systolic blood pressure rose from 30mmHg at the beginning of the procedure to 90mmHg after the embolisation, which took 20 minutes to perform.
Case courtesy of Dr Ronan Ryan, SVUH Interventional Radiologist.