Common duct calculus – multimodality imaging
It is often difficult to identify distal common duct calculi on ultrasound as gas in the duodenum, anterior to the duct, frequently obscures it. However this is an example of a case where the common duct calculus was clearly demonstrated.
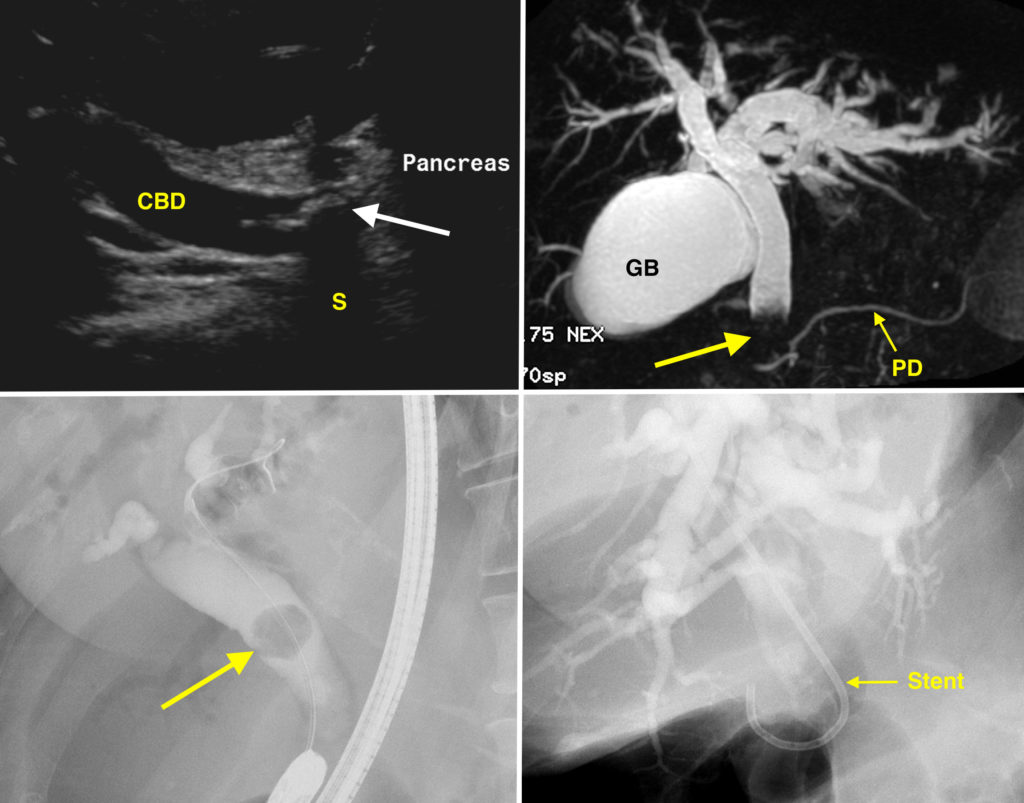
This 60 year old woman presented to the ED with right upper quadrant pain and jaundice. Ultrasound (which should always be the first imaging study in the work-up of a patient with this history) showed a dilated common bile duct (CBD in the top left image), caused by a large calculus (arrow) in the distal aspect of the duct at the level of the pancreas. The CBD measured over 10mm in this case – the normal range is up to 6 mm. As is the case with gallstones in the gallbladder, a typical feature of common duct calculi is that they are echogenic and cause an ‘acoustic shadow’ behind them, where the sound waves do not penetrate (S).
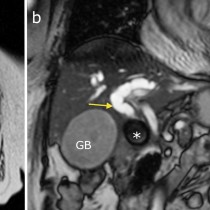
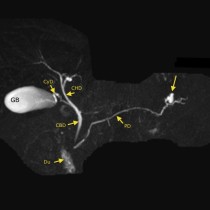
This patient went on to have an MRCP (magnetic resonance cholangiopancreatography) to assess for additional calculi in the biliary tree prior to proceeding to ERCP. The MRCP image, top right, shows the solitary calculus as a filling defect in the distal CBD (arrow). The gallbladder (GB) and normal pancreatic duct (PD) are also labelled). Note how dilated the CBD and the intrahepatic ducts are.
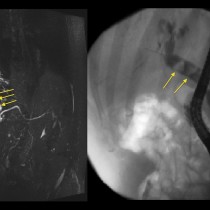
An ERCP was then performed. The bottom left image shows the endoscope in place and that a wire has been advanced up the CBD beyond the large filling defect (arrow) that represents the calculus. A sphincterotomy was performed, the stone was extracted and a plastic CBD stent was inserted (bottom right image).