Acute cholecystitis on CT
Ultrasound should always be your first-line imaging investigation when acute cholecystitis is suspected, however we frequently make the diagnosis on abdominal CT.
The CT may have been performed because the clinician suspects an alternative diagnosis, for example appendicitis, or because the patient’s abdomen is difficult to assess (for example, due to obesity as in this case, or because the patient is unconscious for some other reason).
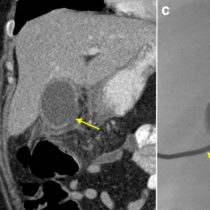
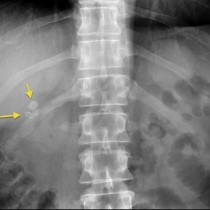
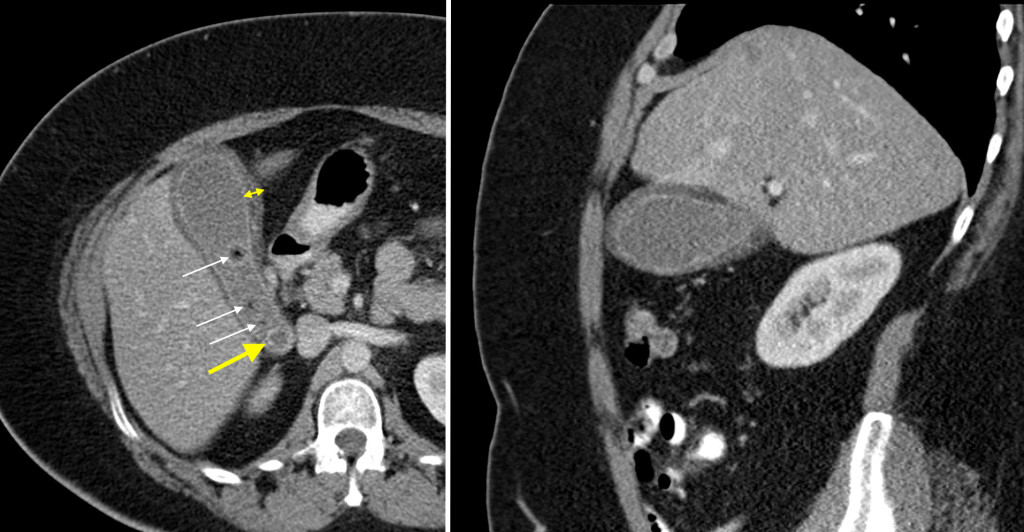
In this example, you will notice how thick the subcutaneous fat is. The clinicians were uncertain as to the cause of this young woman’s abdominal pain, noting that she was diffusely tender. On the transverse image on the left, you can see the thickened, oedematous gallbladder wall (indicated by the double-headed arrow). There are multiple gallbladder calculi (white arrows), one of which looks like it’s stuck in the gallbladder neck (large yellow arrow) and was the cause of the patient’s acute cholecystitis. The gallbladder wall is also well seen on the sagittal image on the right.
In many cases of acute cholecystitis, the gallbladder calculi will not be visible on CT and the gallbladder wall thickening will not be as convincing as this example. In cases where we suspect, but are unsure of, a diagnosis of acute cholecystitis on the basis of a CT we routinely recommend in the report that an ultrasound be performed for confirmation.
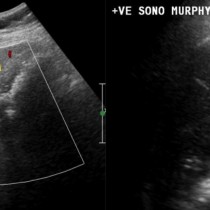
The classical sonographic features of acute cholecystitis are: gallbladder distension, calculi, gallbladder wall thickening >3mm, hyperaemia of the gallbladder wall on Doppler, oedema around the gallbladder (‘pericholecystic oedema’) and a sonographic Murphy’s sign (where the ultrasonographer checks whether the patient is tender while pushing the ultrasound probe over the gallbladder).