Rigler’s sign in small bowel obstruction
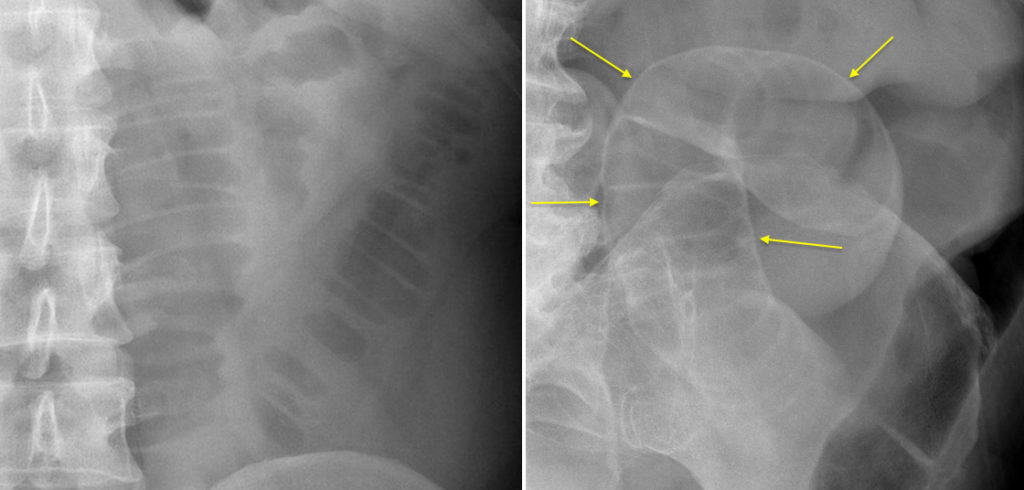
A particularly nice example of Rigler’s sign (also known as the ‘double-wall sign’) is shown here.
The image on the left is from a patient with uncomplicated small bowel obstruction secondary to Crohn disease – note how only the inner (luminal) side of the bowel wall is visible as there is gas in the lumen to outline it. On the right-hand image, taken from the supine PFA of an elderly patient with perforation due to small bowel obstruction, there is gas in the lumen and in the peritoneal cavity so we can see both sides of the wall clearly (arrows). In both cases, the valvulae conniventes are visible extending across the full width of the dilated bowel lumen, confirming that this represents small bowel rather than colon.
A sizeable volume of intraperitoneal gas is required before Rigler’s sign becomes visible on a PFA, therefore it is not a commonly encountered radiographic sign – the erect CXR remains much more sensitive for small volume pneumoperitoneum. The sensitivity of an erect CXR for pneumoperitoneum depends on the source of the perforation. For example, it has a sensitivity of over 90% in perforation of the stomach or duodenum, but drops to 40% for perforation of the colon. The overall sensitivity for all sources of perforation has been reported to be up to 89%1.
Reference:
- Effectiveness of plain radiography in detecting hollow viscus perforation. Emergency Radiology 2012;19:115-119.