Pericardial effusion – CXR and CT
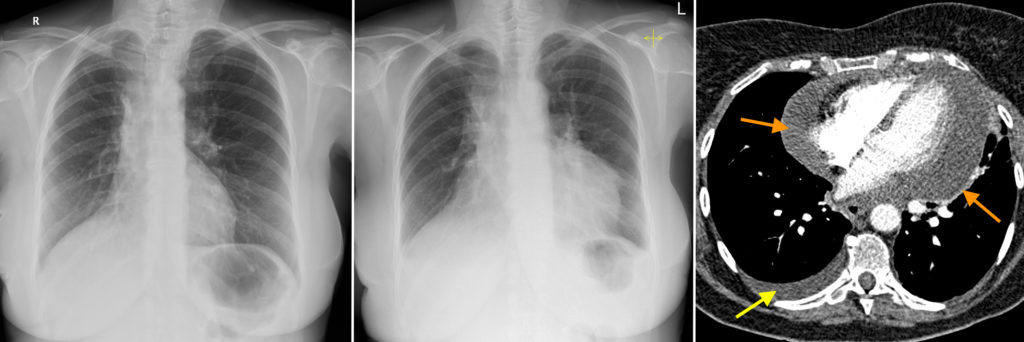
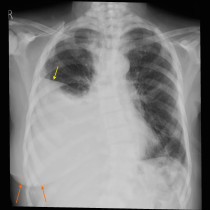
This woman in her 60s has a history of lung cancer for which she had a previous right lower lobectomy. The CXR on the left was a routine follow-up study performed when she attended the oncology outpatient department, at which time she was asymptomatic. You will notice that there is evidence of the previous lobectomy, with signs of volume loss in the right hemithorax – the heart, mediastinum and trachea are deviated to the right, and the right hemidiaphragm is elevated. Note the normal heart size (the cardiothoracic ratio is much lower than 50%).
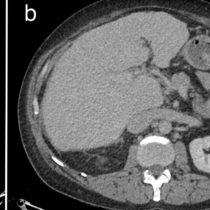
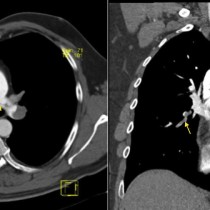
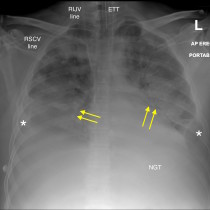
Four months later, the patient presented to the ED with dyspnoea and chest pain that was pleuritic in nature. The provisional diagnosis was that she had had a PE, so a CXR and then a CT pulmonary angiogram (CTPA) were requested. However, you will notice on the CXR, middle image, that the previously-normal heart shadow is now moderately enlarged. The CTPA, right, showed no PE. It also shows that the cardiac chambers are actually normal in size but the apparent cardiomegaly is due to a very large pericardial effusion (orange arrows). There is also a small right pleural effusion (yellow arrow). The pericardial effusion was drained surgically, and cytological analysis of the drained fluid confirmed the suspicion that it was due to metastatic disease.
Pericardial effusions are classically described as causing globular, featureless enlargement of the heart shadow, as in this case. The clue to the diagnosis in this example was the fact that we had a recent prior normal CXR available for review, but of course in reality additional imaging with echocardiography is usually performed to confirm a suspected pericardial effusion.
Potential causes of pericardial effusion include:
- Infection (viral, bacterial, tuberculous)
- Connective tissue disease, e.g. SLE
- Malignancy – primary (mesothelioma) or metastatic
- Myocardial infarction
- Uraemia