Tracheal shift on CXR
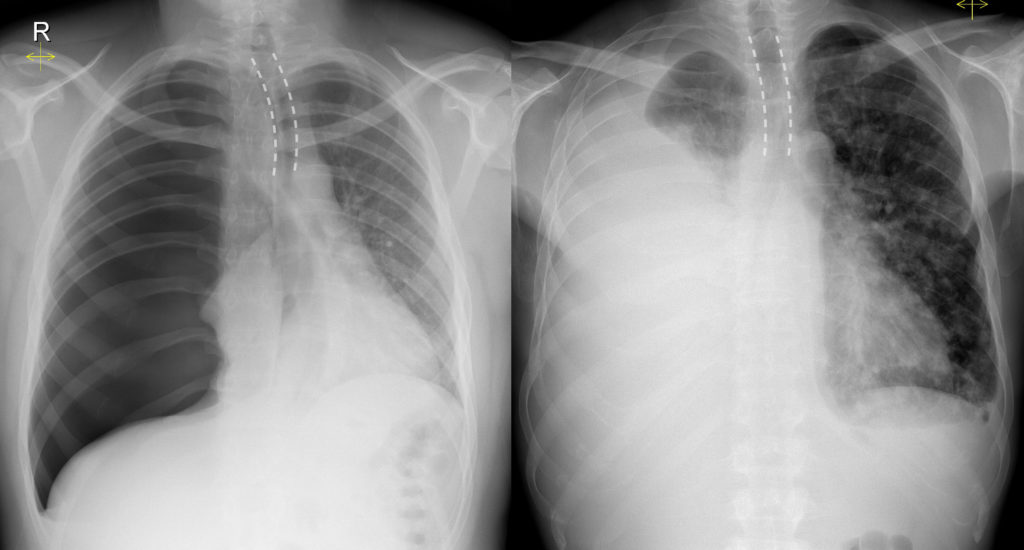
This image shows two chest x-rays in different patients, both showing dramatic examples of tracheal shift.
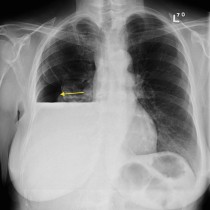
On the left is a 25 year old man who presented to ED with acute chest pain and shortness of breath. His CXR (taken on expiration in order to accentuate the clinically-suspected pneumothorax – the reason for this is explained here), shows a massive right-sided tension pneumothorax with shift of the trachea (outlined by the dashed line) to the left. The heart is also displaced to the left. Note the hyperlucency of the right hemithorax and the absence of any lung markings on this side.
The right-hand image also shows tracheal shift, however this patient was in his 70s and had a background of lung cancer. In this case, the tracheal displacement is due to a massive right pleural effusion, opacifying almost the entire right hemithorax. This was a malignant pleural effusion caused by pleural metastases. If you look carefully you will see multiple nodules throughout the left lung, which were also metastases, plus a small left pleural effusion.
Normally, the trachea is located in the midline at the level of the clavicles, often deviating slightly to the right more inferiorly at the level of the aortic arch.
As a reminder, the causes of tracheal displacement include the following:
Causes of displacement AWAY from the side of the pathology:
- Pneumothorax
- Pleural effusion
- Mediastinal neoplasm including lymphoma, lymphadenopathy, thymic tumour, germ cell tumour
- Retrosternal goitre
Causes of displacement TOWARDS the side of the pathology:
- Apical lung fibrosis (for example, due to TB or prior radiotherapy)
- Collapse of one or more lung segments, for example due to bronchial obstruction by tumour
- Previous pneumonectomy
Occasionally, in a patient with lung cancer and a large malignant pleural effusion, there will be such severe collapse of the underlying lung on the same side due to bronchial obstruction by tumour that the tracheal/mediastinal shift will, paradoxically, be towards the side of the effusion.
It is also worth noting that large mediastinal masses that extend around both sides of the trachea may allow it to remain central, however in this setting they will often cause tracheal narrowing which is also detectable on a CXR.