Felty syndrome
Here is an example of Felty syndrome, which is the triad of rheumatoid arthritis, splenomegaly and neutropenia.
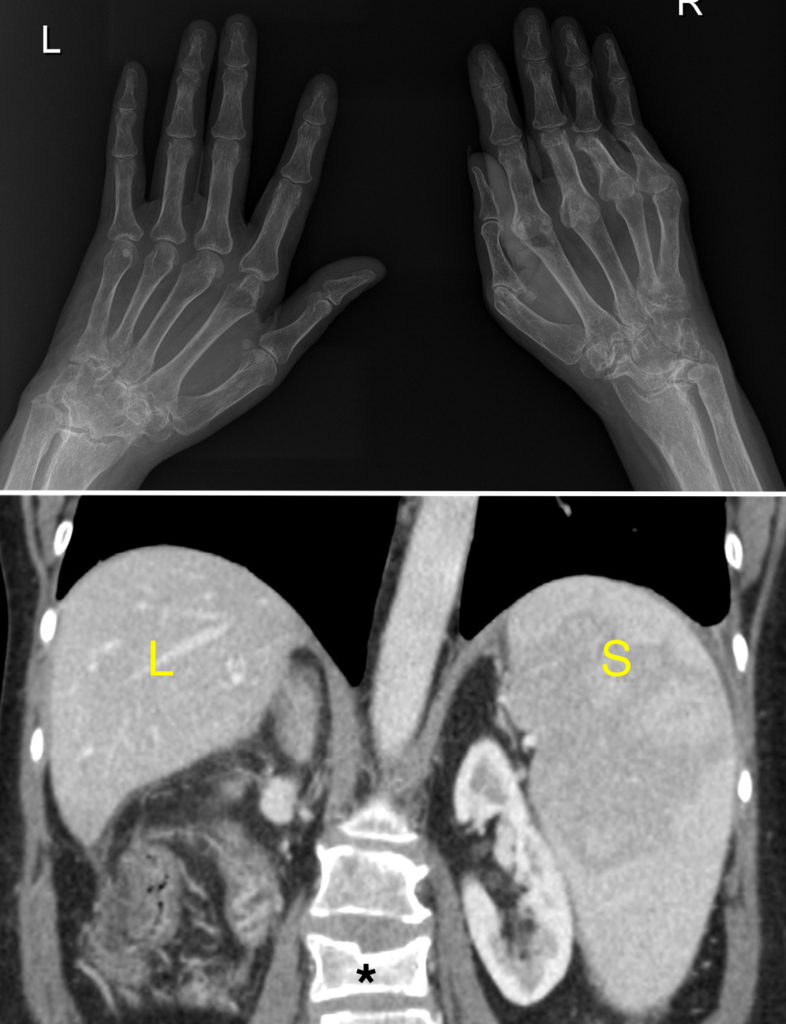
The hand radiographs show advanced changes of rheumatoid arthritis, although they are not typical of the disease as the arthropathy is not symmetrical. On the left, the changes are essentially confined to the wrist – notice how all of the carpal bones have fused together (ankylosis). On the right, it is the MCP joints that are predominantly affected – the joint spaces are obliterated and there is erosion of the bases of the proximal phalanges.
You will recall that rheumatoid arthritis classically causes a ‘proximal, symmetrical arthropathy’, however the symmetry is not always seen. Its proximal distribution is, however, always the case – the distal interphalangeal joints are never involved in rheumatoid arthritis.
The coronal CT image on the bottom shows the normal liver, L, with a very enlarged spleen, S.
Also present is a compression fracture of the L3 vertebra, (*). Patients with rheumatoid arthritis are prone to osteoporotic fractures like this, particularly if they have undergone longterm steroid therapy.
Felty syndrome is uncommon and usually develops many years after the patient has been diagnosed with rheumatoid arthritis. It is more common in rheumatoid patients who have extra-articular manifestations of the disease such as rheumatoid nodules, vasculitis or lymphadenopathy. Patients with Felty syndrome may present with recurrent bacterial pneumonia or other infections, or occasionally with left upper quadrant pain due to splenic infarcts. Although CT was ordered in this case because of the concern of concomitant liver disease that can potentially develop in Felty syndrome, splenomegaly is easily diagnosed with ultrasound which should be the preferred modality if splenic size is the only clinical question you need answered.